1
Introduction
1 min•103 words
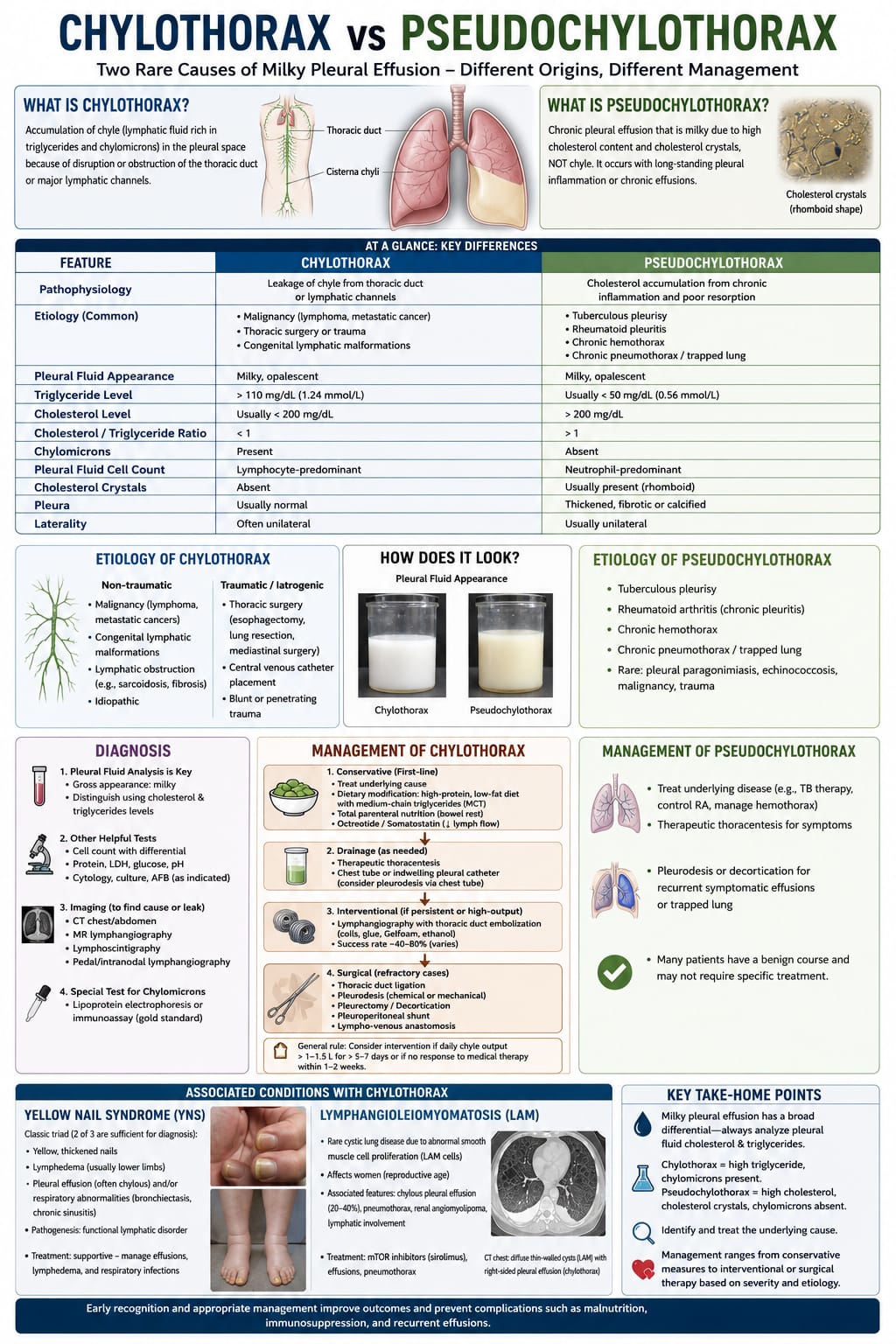
When confronting a pleural effusion with a macroscopically "milky" or opalescent appearance, clinicians frequently face a diagnostic dilemma. A milky presentation is not pathognomonic for a single disease process; rather, it represents two distinct pathophysiological entities with entirely different origins and contrasting treatment pathways: Chylothorax and Pseudochylothorax (also known as cholesterol pleurisy).
Differentiating between these two rare forms of lipid-rich effusions is critically important. Misdiagnosis can lead to inappropriate interventions, ranging from unnecessary, aggressive thoracic surgeries to the mismanagement of underlying chronic infections or systemic autoimmune conditions. A precise biochemical appraisal of the pleural fluid is the cornerstone of making an accurate diagnosis.
Differentiating between these two rare forms of lipid-rich effusions is critically important. Misdiagnosis can lead to inappropriate interventions, ranging from unnecessary, aggressive thoracic surgeries to the mismanagement of underlying chronic infections or systemic autoimmune conditions. A precise biochemical appraisal of the pleural fluid is the cornerstone of making an accurate diagnosis.
2
Background & Pathophysiology
2 min•343 words
The fundamental divergence between chylothorax and pseudochylothorax lies within their underlying mechanical and cellular pathogenesis.
1. Chylothorax
A chylothorax results from the direct anatomical disruption, leakage, or obstruction of the thoracic duct or its primary lymphatic channels. This structural failure allows chyle—a lymphatic fluid rich in long-chain triglycerides and chylomicrons absorbed from the intestinal tract—to flood directly into the pleural space.
Non-Traumatic Etiologies: Primarily driven by mediastinal malignancies such as lymphoma or metastatic carcinoma. It can also be caused by non-malignant lymphatic obstructions like sarcoidosis, retroperitoneal fibrosis, or congenital lymphatic malformations.
Traumatic / Iatrogenic Etiologies: Frequently occurs as a severe complication of cardiothoracic or mediastinal surgeries (e.g., esophagectomy, lung resection), blunt or penetrating thoracic trauma, or central venous catheter misplacement.
2. Pseudochylothorax
Conversely, a pseudochylothorax does not involve the thoracic duct or lymphatic leakage. Instead, it is caused by the chronic, long-standing accumulation of cholesterol within a long-standing, unresorbed pleural effusion trapped inside a thickened, fibrotic, or calcified pleural membrane. Over months or years, cellular lysis of erythrocytes and neutrophils within the stagnant fluid releases structural lipids, which transform into free cholesterol crystals due to poor pleural resorption.
Common Etiologies: Classically driven by tuberculous pleurisy, severe rheumatoid pleuritis (chronic rheumatoid arthritis), chronic hemothorax, or a long-standing trapped lung secondary to chronic pneumothorax.
Rare Etiologies: Pleural paragonimiasis, echinococcosis, or underlying low-grade malignancies.
Biochemical and Cellular Differentiation
CHYLOTHORAX vs. PSEUDOCHYLOTHORAX (Key Differences)
PATHOPHYSIOLOGY
Chylothorax: Leakage of chyle from thoracic duct or lymphatic channels
Pseudochylothorax: Cholesterol accumulation from chronic inflammation and poor resorption
PLEURAL FLUID APPEARANCE
Chylothorax: Milky, opalescent
Pseudochylothorax: Milky, opalescent
TRIGLYCERIDE LEVEL
Chylothorax: High, greater than 110 mg/dL (1.24 mmol/L)
Pseudochylothorax: Usually low, less than 50 mg/dL (0.56 mmol/L)
CHOLESTEROL LEVEL
Chylothorax: Usually low, less than 200 mg/dL
Pseudochylothorax: High, greater than 200 mg/dL
CHOLESTEROL / TRIGLYCERIDE RATIO
Chylothorax: Less than 1
Pseudochylothorax: Greater than 1
CHYLOMICRONS
Chylothorax: Present
Pseudochylothorax: Absent
PLEURAL FLUID CELL COUNT
Chylothorax: Lymphocyte-predominant
Pseudochylothorax: Neutrophil-predominant
CHOLESTEROL CRYSTALS
Chylothorax: Absent
Pseudochylothorax: Usually present (rhomboid-shaped)
PLEURA MORPHOLOGY
Chylothorax: Usually normal
Pseudochylothorax: Thickened, fibrotic, or calcified
LATERALITY
Chylothorax: Often unilateral
Pseudochylothorax: Usually unilateral
1. Chylothorax
A chylothorax results from the direct anatomical disruption, leakage, or obstruction of the thoracic duct or its primary lymphatic channels. This structural failure allows chyle—a lymphatic fluid rich in long-chain triglycerides and chylomicrons absorbed from the intestinal tract—to flood directly into the pleural space.
Non-Traumatic Etiologies: Primarily driven by mediastinal malignancies such as lymphoma or metastatic carcinoma. It can also be caused by non-malignant lymphatic obstructions like sarcoidosis, retroperitoneal fibrosis, or congenital lymphatic malformations.
Traumatic / Iatrogenic Etiologies: Frequently occurs as a severe complication of cardiothoracic or mediastinal surgeries (e.g., esophagectomy, lung resection), blunt or penetrating thoracic trauma, or central venous catheter misplacement.
2. Pseudochylothorax
Conversely, a pseudochylothorax does not involve the thoracic duct or lymphatic leakage. Instead, it is caused by the chronic, long-standing accumulation of cholesterol within a long-standing, unresorbed pleural effusion trapped inside a thickened, fibrotic, or calcified pleural membrane. Over months or years, cellular lysis of erythrocytes and neutrophils within the stagnant fluid releases structural lipids, which transform into free cholesterol crystals due to poor pleural resorption.
Common Etiologies: Classically driven by tuberculous pleurisy, severe rheumatoid pleuritis (chronic rheumatoid arthritis), chronic hemothorax, or a long-standing trapped lung secondary to chronic pneumothorax.
Rare Etiologies: Pleural paragonimiasis, echinococcosis, or underlying low-grade malignancies.
Biochemical and Cellular Differentiation
CHYLOTHORAX vs. PSEUDOCHYLOTHORAX (Key Differences)
PATHOPHYSIOLOGY
Chylothorax: Leakage of chyle from thoracic duct or lymphatic channels
Pseudochylothorax: Cholesterol accumulation from chronic inflammation and poor resorption
PLEURAL FLUID APPEARANCE
Chylothorax: Milky, opalescent
Pseudochylothorax: Milky, opalescent
TRIGLYCERIDE LEVEL
Chylothorax: High, greater than 110 mg/dL (1.24 mmol/L)
Pseudochylothorax: Usually low, less than 50 mg/dL (0.56 mmol/L)
CHOLESTEROL LEVEL
Chylothorax: Usually low, less than 200 mg/dL
Pseudochylothorax: High, greater than 200 mg/dL
CHOLESTEROL / TRIGLYCERIDE RATIO
Chylothorax: Less than 1
Pseudochylothorax: Greater than 1
CHYLOMICRONS
Chylothorax: Present
Pseudochylothorax: Absent
PLEURAL FLUID CELL COUNT
Chylothorax: Lymphocyte-predominant
Pseudochylothorax: Neutrophil-predominant
CHOLESTEROL CRYSTALS
Chylothorax: Absent
Pseudochylothorax: Usually present (rhomboid-shaped)
PLEURA MORPHOLOGY
Chylothorax: Usually normal
Pseudochylothorax: Thickened, fibrotic, or calcified
LATERALITY
Chylothorax: Often unilateral
Pseudochylothorax: Usually unilateral
3
Diagnosis & Workup
1 min•136 words
Pleural Fluid Analysis (The Diagnostic Gold Standard): Evaluate the gross appearance. If the fluid remains milky after centrifugation, analyze the absolute cholesterol and triglyceride levels. If triglyceride levels are indeterminate (between 50 and 110 mg/dL), ordering a lipoprotein electrophoresis or immunoassay to detect the explicit presence of chylomicrons serves as the diagnostic gold standard for confirming a chylothorax.
Microscopic Crystal Examination: Perform light microscopy on the fluid. The detection of classic rhomboid-shaped cholesterol crystals confirms a pseudochylothorax.
Standard Effusion Workup: Track cell count with differential, total protein, LDH, glucose, pH, fluid cytology, bacterial cultures, and Acid-Fast Bacilli (AFB) stains/cultures to screen for underlying tuberculosis or rheumatoid disease.
Targeted Imaging: For confirmed chylothorax, utilize CT scans of the chest and abdomen, MR lymphangiography, lymphoscintigraphy, or pedal/intranodal lymphangiography to localize the precise site of the anatomical lymphatic leak.
Microscopic Crystal Examination: Perform light microscopy on the fluid. The detection of classic rhomboid-shaped cholesterol crystals confirms a pseudochylothorax.
Standard Effusion Workup: Track cell count with differential, total protein, LDH, glucose, pH, fluid cytology, bacterial cultures, and Acid-Fast Bacilli (AFB) stains/cultures to screen for underlying tuberculosis or rheumatoid disease.
Targeted Imaging: For confirmed chylothorax, utilize CT scans of the chest and abdomen, MR lymphangiography, lymphoscintigraphy, or pedal/intranodal lymphangiography to localize the precise site of the anatomical lymphatic leak.
4
Management
3 min•455 words
MANAGEMENT OF CHYLOTHORAX
Management follows a step-up protocol based on daily chyle output volumes:
First-Line Conservative Therapy
Treat the underlying cause (such as chemotherapy for lymphoma). Implement strict dietary modification consisting of a high-protein, low-fat diet supplemented with Medium-Chain Triglycerides (MCT). MCTs bypass the standard intestinal lymphatic system and enter the portal venous circulation directly, reducing chyle flow. If this fails, transition the patient to complete bowel rest using Total Parenteral Nutrition (TPN) paired with Octreotide or Somatostatin infusions to actively decrease splanchnic and lymphatic blood flow.
Drainage
Perform therapeutic thoracentesis or place a standard chest tube or indwelling pleural catheter as needed to relieve dyspnea. Pleurodesis can be considered via the chest tube if the leak persists.
Interventional Lymphatic Embolization
For persistent or high-output leaks, pursue lymphangiography paired with thoracic duct embolization using coils, glue, Gelfoam, or ethanol (success rates range from 40% to 80%).
Surgical Intervention
For refractory cases—defined by a general rule of a daily chyle output greater than 1.0 to 1.5 Liters for more than 5 to 7 days, or a complete lack of response to conservative medical therapy within 1 to 2 weeks—prompt surgical intervention is indicated. This includes direct thoracic duct ligation, chemical or mechanical pleurodesis, pleurectomy or decortication, a pleuroperitoneal shunt, or lympho-venous anastomosis.
MANAGEMENT OF PSEUDOCHYLOTHORAX
Because pseudochylothorax does not involve an active lymphatic leak, its management centers entirely on chronic inflammatory control:
Target the Underlying Pathology: Initiate specific anti-tuberculosis therapy for tuberculous pleurisy, optimize disease-modifying antirheumatic drugs (DMARDs) for rheumatoid arthritis, or surgically evacuate a chronic hemothorax.
Symptom Management: Perform intermittent therapeutic thoracentesis strictly to manage respiratory symptoms.
Mechanical Interventions: Pursue chemical pleurodesis or formal surgical decortication if the patient suffers from recurrent symptomatic effusions or a severely restrictive trapped lung. Many patients follow a completely benign course and may require no specific thoracic treatment if they remain asymptomatic.
ASSOCIATED CLINICAL CONDITIONS WITH CHYLOTHORAX
When evaluating a chylothorax of unknown origin, clinicians must screen for two classic underlying systemic conditions:
Yellow Nail Syndrome (YNS)
A rare systemic functional lymphatic disorder. A clinical diagnosis is established when any 2 of its 3 classic triad features are present:
Distinctly yellow, thickened nails.
Chronic, asymmetric lymphedema (predominantly involving the lower limbs).
Pleural effusions (frequently chylous) and/or chronic respiratory abnormalities (such as diffuse bronchiectasis or chronic sinusitis).
Management is supportive, focusing on effusion drainage and managing lymphedema.
Lymphangioleiomyomatosis (LAM)
A rare cystic lung disease driven by abnormal, smooth muscle-like cell proliferation (LAM cells) that almost exclusively affects females of reproductive age. It leads to diffuse, thin-walled parenchymal lung cysts and causes chylous pleural effusions in 20% to 40% of cases due to lymphatic involvement, alongside recurrent pneumothoraces and renal angiomyolipomas. Management involves targeted therapy with mTOR inhibitors such as Sirolimus.
Management follows a step-up protocol based on daily chyle output volumes:
First-Line Conservative Therapy
Treat the underlying cause (such as chemotherapy for lymphoma). Implement strict dietary modification consisting of a high-protein, low-fat diet supplemented with Medium-Chain Triglycerides (MCT). MCTs bypass the standard intestinal lymphatic system and enter the portal venous circulation directly, reducing chyle flow. If this fails, transition the patient to complete bowel rest using Total Parenteral Nutrition (TPN) paired with Octreotide or Somatostatin infusions to actively decrease splanchnic and lymphatic blood flow.
Drainage
Perform therapeutic thoracentesis or place a standard chest tube or indwelling pleural catheter as needed to relieve dyspnea. Pleurodesis can be considered via the chest tube if the leak persists.
Interventional Lymphatic Embolization
For persistent or high-output leaks, pursue lymphangiography paired with thoracic duct embolization using coils, glue, Gelfoam, or ethanol (success rates range from 40% to 80%).
Surgical Intervention
For refractory cases—defined by a general rule of a daily chyle output greater than 1.0 to 1.5 Liters for more than 5 to 7 days, or a complete lack of response to conservative medical therapy within 1 to 2 weeks—prompt surgical intervention is indicated. This includes direct thoracic duct ligation, chemical or mechanical pleurodesis, pleurectomy or decortication, a pleuroperitoneal shunt, or lympho-venous anastomosis.
MANAGEMENT OF PSEUDOCHYLOTHORAX
Because pseudochylothorax does not involve an active lymphatic leak, its management centers entirely on chronic inflammatory control:
Target the Underlying Pathology: Initiate specific anti-tuberculosis therapy for tuberculous pleurisy, optimize disease-modifying antirheumatic drugs (DMARDs) for rheumatoid arthritis, or surgically evacuate a chronic hemothorax.
Symptom Management: Perform intermittent therapeutic thoracentesis strictly to manage respiratory symptoms.
Mechanical Interventions: Pursue chemical pleurodesis or formal surgical decortication if the patient suffers from recurrent symptomatic effusions or a severely restrictive trapped lung. Many patients follow a completely benign course and may require no specific thoracic treatment if they remain asymptomatic.
ASSOCIATED CLINICAL CONDITIONS WITH CHYLOTHORAX
When evaluating a chylothorax of unknown origin, clinicians must screen for two classic underlying systemic conditions:
Yellow Nail Syndrome (YNS)
A rare systemic functional lymphatic disorder. A clinical diagnosis is established when any 2 of its 3 classic triad features are present:
Distinctly yellow, thickened nails.
Chronic, asymmetric lymphedema (predominantly involving the lower limbs).
Pleural effusions (frequently chylous) and/or chronic respiratory abnormalities (such as diffuse bronchiectasis or chronic sinusitis).
Management is supportive, focusing on effusion drainage and managing lymphedema.
Lymphangioleiomyomatosis (LAM)
A rare cystic lung disease driven by abnormal, smooth muscle-like cell proliferation (LAM cells) that almost exclusively affects females of reproductive age. It leads to diffuse, thin-walled parenchymal lung cysts and causes chylous pleural effusions in 20% to 40% of cases due to lymphatic involvement, alongside recurrent pneumothoraces and renal angiomyolipomas. Management involves targeted therapy with mTOR inhibitors such as Sirolimus.
5
Key Pearls & Takeaways
1 min•181 words
Look at the Lipids: Never diagnose a milky effusion by sight alone. Check the triglycerides and cholesterol. A high triglyceride level (>110 mg/dL) with chylomicrons confirms a chylothorax; a high cholesterol level (>200 mg/dL) with rhomboid crystals points to a pseudochylothorax.Check the Pleural Membrane: A normal pleural appearance on imaging points toward an acute chylothorax. A heavily thickened, fibrotic, or calcified pleural line is a diagnostic hallmark of a chronic pseudochylothorax.MCTs Bypass the Leak: In a conservative chylothorax protocol, standard dietary fats must be avoided. Use Medium-Chain Triglycerides (MCTs) because they absorb directly into the portal vein, allowing you to nourish the patient without increasing thoracic duct chyle output.The Surgical Cut-off Rule: Do not let a chylothorax leak indefinitely. If daily chest tube output exceeds 1 to 1.5 Liters for more than 5 to 7 days despite TPN and octreotide, halt conservative management and consult thoracic surgery for duct ligation.Think Tuberculosis and RA in Pseudochylothorax: A pseudochylothorax means fluid has been trapped for a long time. Always screen the fluid for Mycobacterium tuberculosis and evaluate the patient for underlying rheumatoid arthritis.
0/5