Preparing your experience, please wait…
K
Home Spot Dx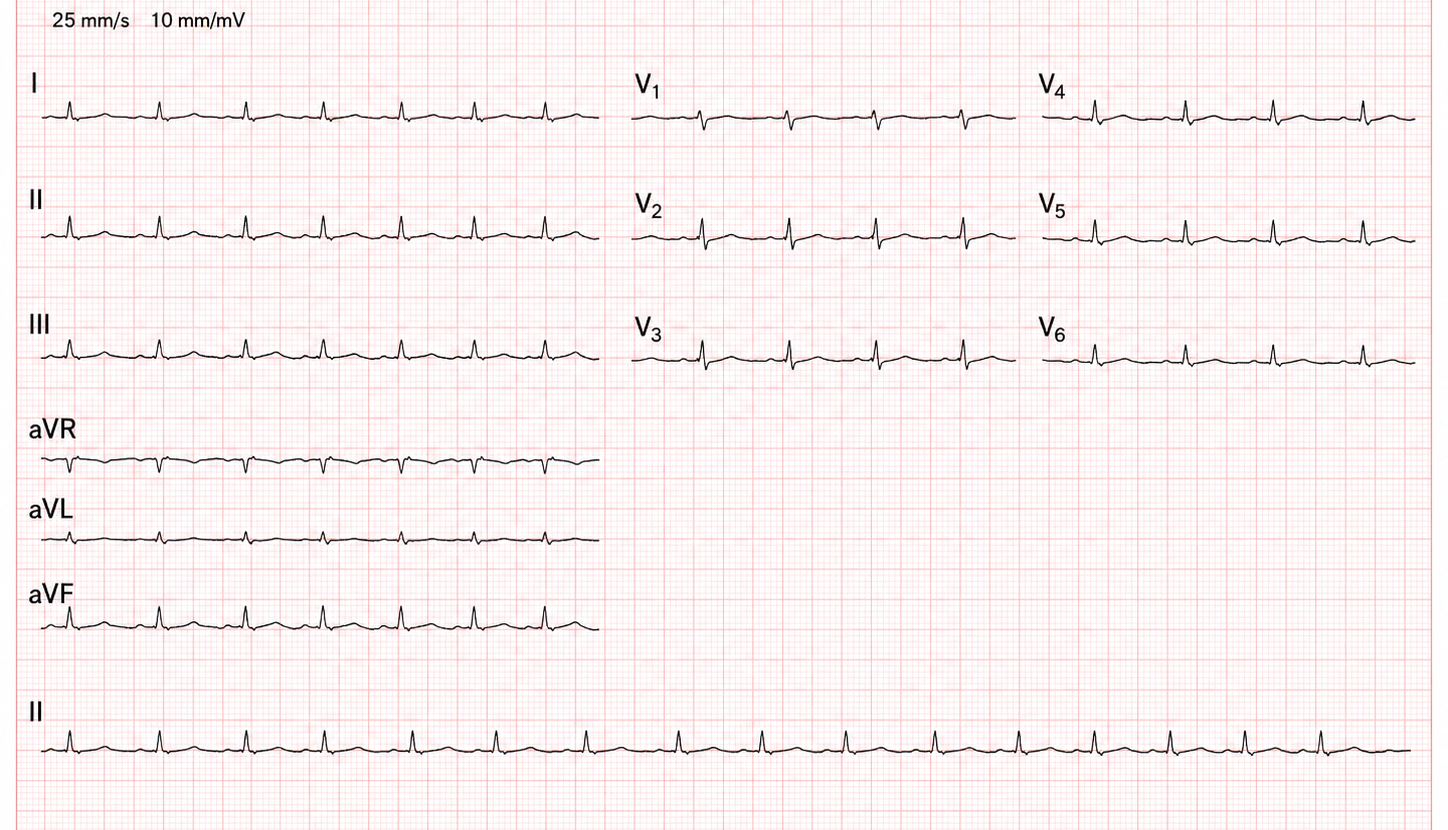

Spot Dx
Clinical reasoning prompts
Brief cases to sharpen your diagnostic reasoning. Think through the question, reveal the answer, and join the WhatsApp discussion.
Nutrition
2/F with swelling of limbs, skin peeling, and 'miserable' mood
A 2-year-old girl is brought to a health center because her legs and face have become swollen over the last month. Her mother reports she is 'always crying' and has lost her appetite for food. On examination, she has pitting edema up to her knees, thin reddish hair, and dark skin lesions on her thighs. Her heart rate is 85 bpm and her temperature is 35.5°C.
In a child with SAM, standard vital sign thresholds for infection (like tachycardia or fever) may be absent; bradycardia and hypothermia are late indicators of severe sepsis or electrolyte derangement.
Cardiology
45/F with acute chest pain and dyspnea
A 45-year-old female, who had recently been evaluated at a local clinic for symptoms of a febrile illness, presents to the emergency department with acute shortness of breath and chest pain that worsens with lying down. She reports a 2-day history of fever and dry cough, but no one with similar symptoms at home. Clinical examination reveals a blood pressure of 90/60 mmHg, a heart rate of 115 bpm, and an elevated jugular venous pressure (JVP). Heart sounds (1 & 2) are heard, but distant. An ECG shows low voltage QRS complexes, but no obvious ischemic changes. Troponin levels are mildly elevated, but not significantly so for her presentation. She has no history of heart disease, but her family reports a delay in seeking medical care due to financial constraints.
In resource-limited settings, bedside ultrasound can be a valuable tool for rapid diagnosis of life-threatening conditions like cardiac tamponade, allowing for timely intervention and potentially improving patient outcomes. However, as it is not always available, high index of suspicion should call for early escalation if unable.
Internal Medicine
Cough and weight loss in a 34-year-old farmer
A 34-year-old tobacco farmer from Mukono presents with a 6-week history of productive cough, night sweats, and unintentional 8 kg weight loss. He has no prior medical history. On examination: BMI 17.2, bilateral coarse crackles in the upper zones, no peripheral lymphadenopathy.
Upper-zone crackles + constitutional symptoms in a high-burden setting = think TB first, not pneumonia.