1
Introduction
1 min•107 words
Chronic Obstructive Pulmonary Disease (COPD) has traditionally been viewed as a non-reversible, progressive inflammatory airway disease primarily driven by neutrophilic inflammation secondary to chronic cigarette smoke exposure or environmental pollutants. For decades, pharmacological management relied strictly on escalating combinations of inhaled bronchodilators and non-targeted inhaled corticosteroids aimed entirely at symptomatic relief and non-specific reduction of acute exacerbation rates.
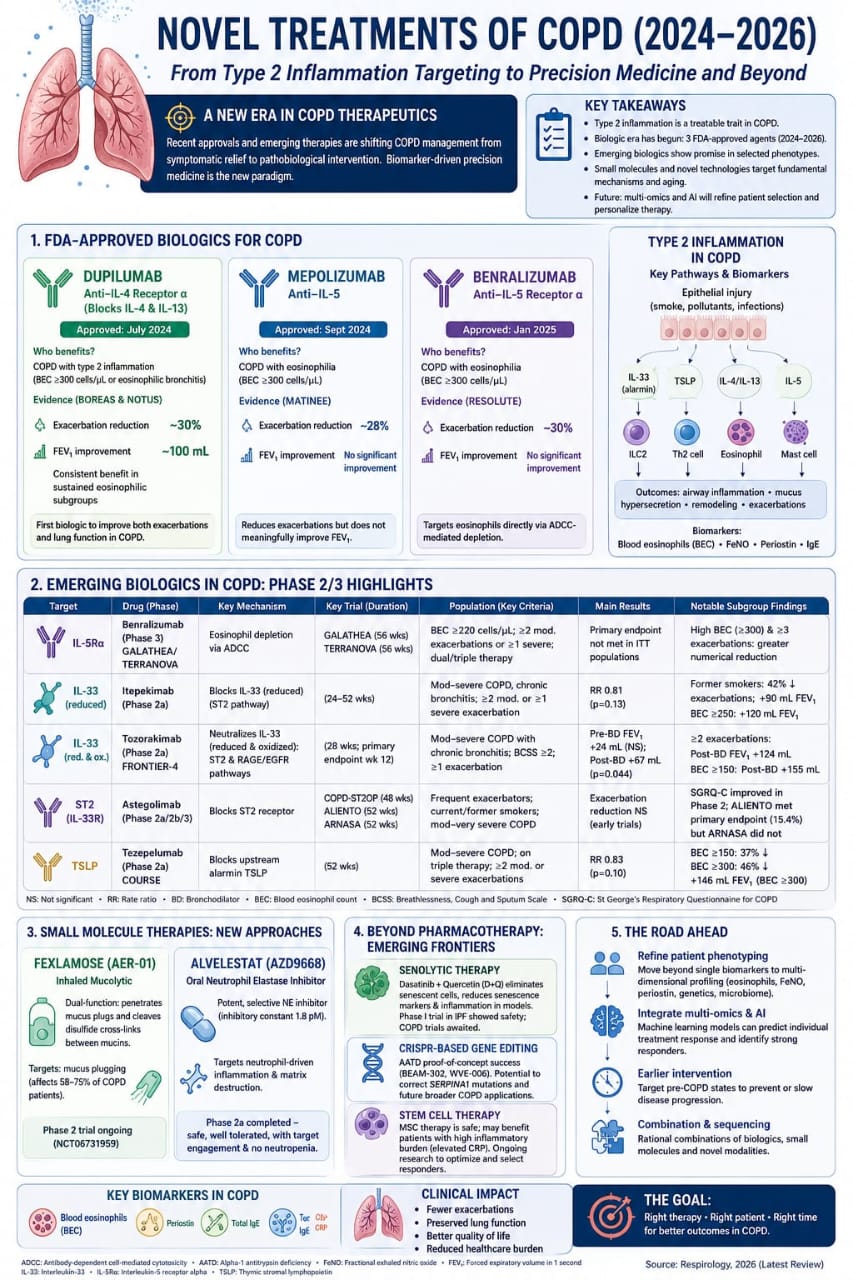
However, the medical community has entered a new era in COPD therapeutics spanning 2024 to 2026. Management is rapidly shifting from broad symptomatic relief toward precise, pathobiological interventions. Biomarker-driven precision medicine represents the modern clinical paradigm, allowing for the targeted matching of specific molecular phenotypes with revolutionary biologic therapies.
However, the medical community has entered a new era in COPD therapeutics spanning 2024 to 2026. Management is rapidly shifting from broad symptomatic relief toward precise, pathobiological interventions. Biomarker-driven precision medicine represents the modern clinical paradigm, allowing for the targeted matching of specific molecular phenotypes with revolutionary biologic therapies.
2
Background & Pathophysiology
1 min•178 words
A major milestone in understanding chronic airway disease is the recognition of Type 2 (T2) inflammation as a distinct, treatable trait in a significant subset of COPD patients. Chronic epithelial injury triggered by smoke, pollutants, or recurrent infections initiates an upstream inflammatory signaling cascade. Damaged epithelial cells release "alarmins," which include Interleukin-33 (IL-33) and Thymic Stromal Lymphopoietin (TSLP).
These alarmins stimulate Type 2 Innate Lymphoid Cells (ILC2) and T-helper 2 (Th2) cells, which downstream drive the heavy production of key Type 2 interleukins, specifically IL-4, IL-13, and IL-5.
IL-4 and IL-13 signaling networks are heavily involved in goblet cell hyperplasia, driving chronic mucus hypersecretion, tissue remodeling, and smooth muscle hyper-reactivity.
IL-5 operates as the primary cytokine responsible for the differentiation, maturation, activation, and survival of eosinophils.
When these pathways are chronically upregulated, eosinophils and mast cells infiltrate the bronchial mucosa, resulting in persistent tissue remodeling, hyper-responsiveness, and frequent, severe respiratory exacerbations. Evaluating this specific T2 pathway relies on identifiable peripheral biomarkers, including an elevated blood eosinophil count (BEC), fractional exhaled nitric oxide (FeNO), periostin, and total serum IgE.
These alarmins stimulate Type 2 Innate Lymphoid Cells (ILC2) and T-helper 2 (Th2) cells, which downstream drive the heavy production of key Type 2 interleukins, specifically IL-4, IL-13, and IL-5.
IL-4 and IL-13 signaling networks are heavily involved in goblet cell hyperplasia, driving chronic mucus hypersecretion, tissue remodeling, and smooth muscle hyper-reactivity.
IL-5 operates as the primary cytokine responsible for the differentiation, maturation, activation, and survival of eosinophils.
When these pathways are chronically upregulated, eosinophils and mast cells infiltrate the bronchial mucosa, resulting in persistent tissue remodeling, hyper-responsiveness, and frequent, severe respiratory exacerbations. Evaluating this specific T2 pathway relies on identifiable peripheral biomarkers, including an elevated blood eosinophil count (BEC), fractional exhaled nitric oxide (FeNO), periostin, and total serum IgE.
3
Clinical Features
1 min•113 words
The clinical presentation of a patient harboring a Type 2 inflammatory COPD phenotype overlaps significantly with classic COPD, but is characterized by a higher frequency of exacerbations and a pattern that may mimic features of asthma (asthma-COPD overlap). To identify patients who will truly benefit from advanced precision therapeutics, clinicians must rely on objective biomarker cut-offs rather than clinical history alone. The standard threshold identifying a prominent Type 2 inflammatory or eosinophilic endotype is a Blood Eosinophil Count (BEC) >= 300 cells/uL. Patients presenting with this specific biochemical profile, especially those with a history of recurrent exacerbations or eosinophilic bronchitis despite optimal baseline inhaler therapy, are the prime candidates for targeted biologic interventions.
4
Diagnosis & Workup
1 min•125 words
Fulfilling the modern workup of advanced COPD requires moving beyond standard spirometry to conduct comprehensive molecular phenotyping.
Quantitative Biomarker Mapping: A complete blood count must be reviewed to check the absolute Blood Eosinophil Count. Measuring FeNO and checking serum IgE and periostin levels provide supportive evidence of an active T2 pathway.
Clinical Severity and Exacerbation History Tracking: Document the exact frequency of past exacerbations. Advanced interventions are primarily indicated for patients who continue to experience two or more moderate exacerbations, or at least one severe exacerbation requiring hospitalization, within the preceding 12 months while adherent to standard triple or dual inhaler therapy.
Advanced Phenotyping Framework: The workup is evolving to integrate multi-dimensional profiling, combining blood eosinophils with multi-omics, genetics, and microbiome analysis to personalize therapy.
Quantitative Biomarker Mapping: A complete blood count must be reviewed to check the absolute Blood Eosinophil Count. Measuring FeNO and checking serum IgE and periostin levels provide supportive evidence of an active T2 pathway.
Clinical Severity and Exacerbation History Tracking: Document the exact frequency of past exacerbations. Advanced interventions are primarily indicated for patients who continue to experience two or more moderate exacerbations, or at least one severe exacerbation requiring hospitalization, within the preceding 12 months while adherent to standard triple or dual inhaler therapy.
Advanced Phenotyping Framework: The workup is evolving to integrate multi-dimensional profiling, combining blood eosinophils with multi-omics, genetics, and microbiome analysis to personalize therapy.
5
Management
3 min•410 words
The therapeutic landscape has evolved rapidly with three FDA-approved agents becoming available between 2024 and 2025, alongside promising small molecules and cell-based pipelines.1. FDA-Approved Biologics for COPDDupilumab (Approved July 2024): A monoclonal antibody targeting the Anti-IL-4 Receptor alpha subunit, effectively blocking both the IL-4 and IL-13 pathways. Validated by the landmark BOREAS & NOTUS clinical trials, it is indicated for patients with a BEC >= 300 cells/uL. Dupilumab is the first biologic demonstrated to simultaneously reduce acute exacerbations by approximately 30% and significantly improve lung function, generating a baseline FEV1 improvement of roughly 100 mL.Mepolizumab (Approved September 2024): A monoclonal antibody targeting circulating IL-5 directly. Evaluated in the MATINEE trial, it is indicated for COPD with eosinophilia (BEC >= 300 cells/uL). It achieves an exacerbation reduction of approximately 28%, though it demonstrates no significant improvement in baseline FEV1.Benralizumab (Approved January 2025): A monoclonal antibody targeting the IL-5 Receptor alpha subunit. Backed by the RESOLUTE trial, it targets eosinophils directly via Antibody-Dependent Cell-Mediated Cytotoxicity (ADCC)-mediated depletion. In patients with a BEC >= 300 cells/uL, it reduces exacerbations by roughly 30% but shows no significant improvement in FEV1. Emerging Biologics (Phase 2/3 Highlights). Multiple upstream targets are under evaluation:Tozorakimab & Itepekimab: Target the alarmin IL-33. Tozorakimab neutralizes both reduced and oxidized IL-33 (FRONTIER-4 trial), showing a post-bronchodilator FEV1 improvement of +155 mL in patients with a BEC >= 150 cells/uL and a history of $\ge$ 2 exacerbations.Astegolimab: Blocks the ST2 (IL-33R) receptor, showing exacerbation reductions in early phase 2 trials (COPD-ST2OP, ALIENTO, ARNASA).Tezepelumab: Blocks upstream alarmin TSLP (COURSE trial), demonstrating a 46% reduction in exacerbations and an increase of +146 mL in FEV1 specifically in the subgroup with a BEC >= 300 cells/uL. Novel Small Molecule ApproachesFexlamose (AER-01): An innovative inhaled mucolytic currently in Phase 2 trials. It targets mucus plugging—which affects 58-75% of COPD patients—by penetrating mucus plugs and cleaving disulfide cross-links between mucins.Alvelestat (AZD9668): A potent, selective oral neutrophil elastase inhibitor that completed Phase 2a testing. It specifically targets neutrophil-driven inflammation and matrix destruction without causing neutropenia.4. Advanced Emerging FrontiersBeyond standard pharmacotherapy, the future of COPD care includes:Senolytic Therapy: Combining Dasatinib + Quercetin (D+Q) to selectively eliminate senescent cells, thereby reducing the localized senescence markers and chronic inflammation associated with pulmonary aging.CRISPR-Based Gene Editing: Proof-of-concept studies (BEAM-302, WVE-006) targeting Alpha-1 Antitrypsin Deficiency (AATD) to correct underlying SERPINA1 mutations.Stem Cell Therapy: Mesenchymal Stem Cell (MSC) therapy has demonstrated safety in trials, offering potential benefit to patients with high baseline inflammatory burdens.
6
Key Pearls & Takeaways
1 min•151 words
Biomarkers Dictate Biologics: The modern management of advanced COPD requires a blood eosinophil check. A BEC >= 300 cells/uL is the standard threshold to consider initiating targeted biologic therapy.Dupilumab Clears Both Hurdles: Among the newly approved biologics, Dupilumab is uniquely able to significantly reduce acute exacerbation frequency (approx30%) while simultaneously improving objective lung function (approx 100 mL FEV1 improvement).Anti-IL-5 Reductions are Exacerbation-Specific: Both Mepolizumab and Benralizumab are highly effective at dropping exacerbation rates by roughly 28-30% in eosinophilic phenotypes, but clinicians must note that neither agent significantly improves a patient's baseline FEV1.Watch the Mucus Plugging Pipeline: Small molecules are shifting to address structural deficits. Fexlamose represents an advanced class of inhaled mucolytics designed to chemically dissolve internal disulfide links within mucin plugs.The AI Paradigm: The road ahead involves integrating machine learning and multi-omics profiling to move past single-biomarker assessments, allowing clinicians to predict individual treatment responses before opening a single vial.
0/6