1
Introduction
1 min•107 words
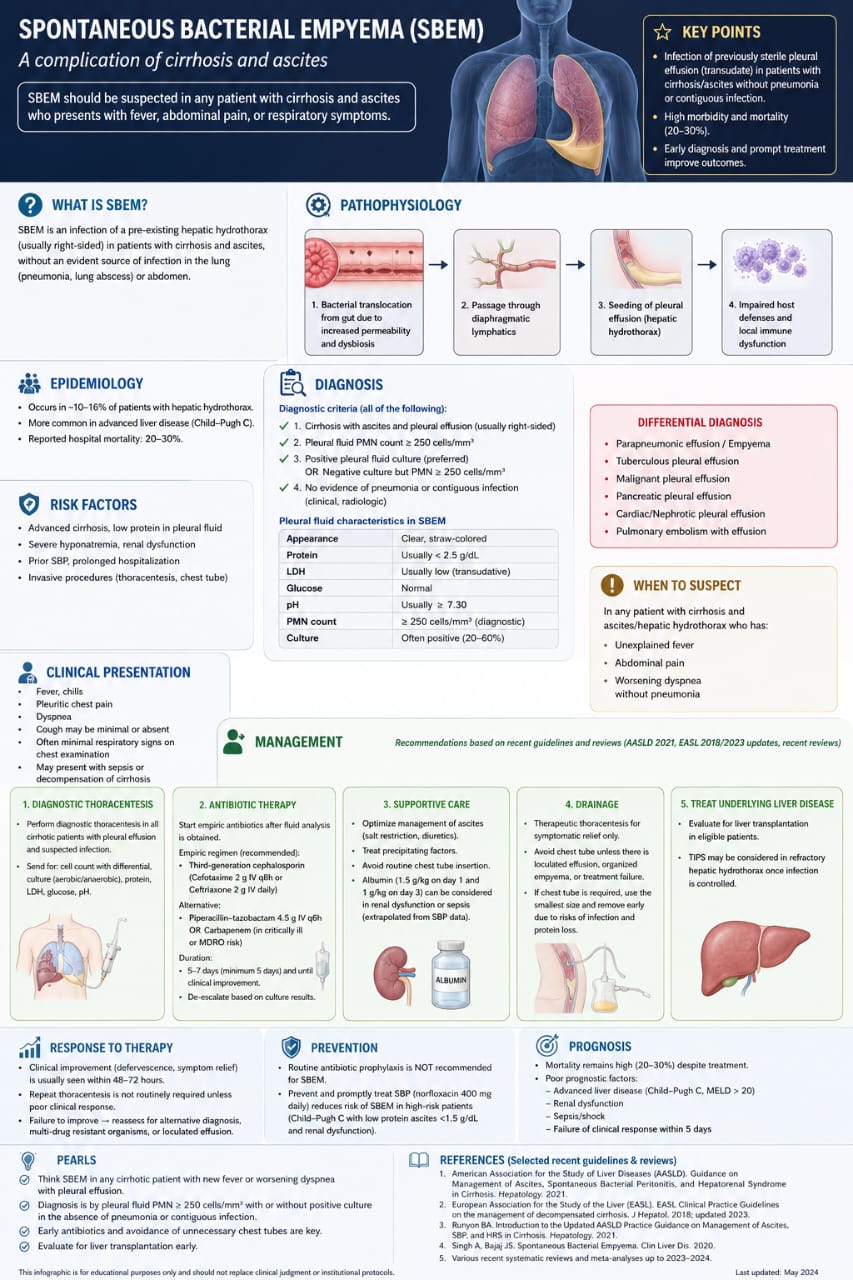
Spontaneous Bacterial Empyema (SBEM) is a severe, often underdiagnosed infectious complication that occurs in patients with advanced cirrhosis and ascites. SBEM is strictly defined as an infection of a pre-existing, sterile hepatic hydrothorax (usually right-sided) without any clinical or radiological evidence of an underlying lung infection (such as pneumonia or a lung abscess) or a contiguous intra-abdominal infection source.
Because its clinical presentation can be remarkably subtle, a high index of clinical suspicion is mandatory. SBEM carries a high hospital morbidity and mortality rate, ranging from 20% to 30%. Early diagnostic recognition and the immediate initiation of targeted therapy are the most critical determinants of patient survival.
Because its clinical presentation can be remarkably subtle, a high index of clinical suspicion is mandatory. SBEM carries a high hospital morbidity and mortality rate, ranging from 20% to 30%. Early diagnostic recognition and the immediate initiation of targeted therapy are the most critical determinants of patient survival.
2
Background & Pathophysiology
2 min•227 words
The development of Spontaneous Bacterial Empyema is intimately linked to the physiological disruptions of portal hypertension and the formation of a hepatic hydrothorax. The step-by-step pathobiological cascade of SBEM involves:Bacterial Translocation: Pathogenic bacteria translocate across the compromised gut mucosa into the mesenteric lymph nodes, heavily driven by increased intestinal permeability and local bacterial dysbiosis inherent to advanced cirrhosis.Microbial Seeding: These bacteria enter the systemic circulation or transdiaphragmatic lymphatics. In patients with a pre-existing hepatic hydrothorax—where peritoneal fluid moves directly into the pleural space through microscopic diaphragmatic defects—the translocated bacteria seed the previously sterile pleural fluid.Immune Dysfunction: Once inside the pleural space, the bacteria proliferate rapidly because the fluid has low protein and compromised opsonic activity. This is further exacerbated by the patient's systemic cirrhotic cardiomyopathy and profound local immune dysfunction, converting a transudative fluid collection into an active, spontaneous empyema.Epidemiology and Risk FactorsSBEM develops in approximately 10% to 16% of patients who possess a baseline hepatic hydrothorax. It is overwhelmingly more common in patients with end-stage, advanced liver disease categorized as Child-Pugh Class C.Established clinical risk factors that predispose a cirrhotic patient to SBEM include:Advanced cirrhosis paired with a low baseline protein level in the pleural fluid (<2.5 g/dL).Severe hyponatremia and underlying renal dysfunction.A prior history of Spontaneous Bacterial Peritonitis (SBP) or prolonged hospitalizations.History of recent invasive thoracic procedures, such as therapeutic thoracentesis or chest tube placements.
3
Clinical Features
1 min•77 words
The clinical hallmarks of SBEM can be non-specific, occasionally manifesting as generalized clinical deterioration rather than localized respiratory distress. Clinicians must actively suspect SBEM in any patient with known cirrhosis and ascites/hepatic hydrothorax who develops:
Unexplained, new-onset fever or chills.
Acute abdominal pain or pleuritic chest pain.
Worsening dyspnea or cough, even when respiratory chest signs are minimal or completely absent.
Sudden worsening of hepatic encephalopathy, acute kidney injury, or unexplained hemodynamic decompensation of their baseline cirrhosis.
Unexplained, new-onset fever or chills.
Acute abdominal pain or pleuritic chest pain.
Worsening dyspnea or cough, even when respiratory chest signs are minimal or completely absent.
Sudden worsening of hepatic encephalopathy, acute kidney injury, or unexplained hemodynamic decompensation of their baseline cirrhosis.
4
Diagnosis & Workup
2 min•235 words
A definitive diagnosis of Spontaneous Bacterial Empyema relies entirely on a prompt diagnostic thoracentesis and strict pleural fluid analysis. Clinicians must never wait for classic signs of pneumonia to validate a pleural tap.1. Mandatory Diagnostic CriteriaTo formally diagnose SBEM, the patient must fulfill all of the following four criteria simultaneously:Documented diagnosis of cirrhosis with ascites and a pre-existing pleural effusion (which is right-sided in the vast majority of cases).A pleural fluid Polymorphonuclear (PMN) cell count >= 250 cells/ml. A positive pleural fluid culture (preferred), OR a negative culture but with a verified PMN count >= 250 cells/ml in the absence of prior antibiotic exposure. Definitive exclusion of pneumonia or any contiguous source of thoracic infection via clinical and radiological evaluation.2. Typical Pleural Fluid Characteristics in SBEMThe background fluid profile of SBEM retains its underlying transudative features despite the active infection, separating it from standard parapneumonic empyemas:Appearance: Clear, straw-colored (unlike the thick, purulent fluid of standard bacterial empyema).Protein Content: Usually low (<2.5 g/dL).LDH Levels: Usually low (transudative background).Glucose & pH: Glucose tracks within normal limits, and pH is usually >= 7.30. Culture Positivity: Fluid cultures are positive in roughly 20% to 60% of cases.3. Differential DiagnosisSBEM must be carefully differentiated from alternative causes of exudative or secondary pleural fluid collections, including:Standard parapneumonic effusion / secondary bacterial empyema (driven by underlying pneumonia).Tuberculous pleural effusion.Malignant pleural effusion.Pancreatic, cardiac, or nephrotic-driven pleural effusions.Pulmonary embolism presenting with a reactive effusion.
5
Management
3 min•446 words
The therapeutic strategy for managing SBEM combines immediate antibiotic coverage, targeted supportive care, and a highly conservative approach to mechanical chest drainage.1. Empiric Antibiotic TherapyEmpiric intravenous antibiotics must be initiated immediately after the diagnostic thoracentesis fluid sample is secured.First-Line Recommended Regimen: A third-generation cephalosporin is the standard of care. Administer Intravenous Cefotaxime (2g given every 8 hours) or Intravenous Ceftriaxone (2g given intravenously every 24 hours).Alternative Regimen: For patients who are critically ill, in septic shock, or at high risk for Multi-Drug Resistant Organisms (MDROs), escalate therapy immediately to Piperacillin-Tazobactam (4.5g IV every 6 hours) or a broad-spectrum Carbapenem (e.g., Meropenem).Duration: Antibiotic therapy must be maintained for a minimum of 5 to 7 days and continued until definitive clinical improvement and defervescence are achieved. De-escalate the antibiotic spectrum as soon as specific culture results become available.2. Essential Supportive Care and Albumin ProtocolOptimize the baseline medical management of ascites using cautious salt restriction and tailored diuretic therapy. Crucially, in line with established SBP treatment parameters, the administration of intravenous Albumin (1.5 g/kg of body weight on Day 1, followed by 1.0 g/kg on Day 3) must be strongly considered, particularly if the patient exhibits signs of worsening renal dysfunction or systemic sepsis, to preserve renal perfusion and reduce the risk of type-1 hepatorenal syndrome.3. Rigid Avoidance of Routine Chest TubesA critical management pearl detailed in "1000306499.jpg" is that routine chest tube insertion is explicitly contraindicated for SBEM. Standard chest tubes must be strictly avoided because they do not improve outcomes in transudative-based spontaneous infections and carry an immense risk of inducing secondary bacterial superinfections, profound protein loss, and mechanical chest wall trauma. Instead, manage fluid-driven dyspnea via intermittent therapeutic thoracentesis. A chest tube should only be considered as an absolute last resort if there is documented loculated empyema fluid, secondary structural organization, or an explicit failure of standard medical therapy. If a chest tube becomes mandatory, utilize the smallest possible size and remove it early.4. Response Tracking and Long-Term PreventionClinical improvement—manifesting as defervescence and symptom relief—is typically observed within 48 to 72 hours of initiating therapy. A repeat thoracentesis is not routinely required unless the patient demonstrates a poor clinical response. If a patient fails to improve within 5 days, clinicians must immediately reassess for an alternative diagnosis, MDROs, or hidden fluid loculation.For long-term management, routine antibiotic prophylaxis is not recommended specifically for SBEM alone. However, preventing and promptly treating standard SBP using oral Norfloxacin (400 mg daily) significantly reduces the secondary incidence of SBEM in high-risk patients who harbor low-protein ascites (<1.5 g/dL) paired with renal or hepatic impairment. Ultimately, eligible patients should be evaluated early for liver transplantation, as SBEM signifies end-stage decompensated liver disease.
6
Key Pearls & Takeaways
1 min•180 words
Think Fluid, Not Just Lungs: Never assume a febrile, dyspneic cirrhotic patient has standard pneumonia. If they have a hepatic hydrothorax, SBEM must be your top differential diagnosis, even if their chest exam and chest X-ray show no parenchymal consolidations.The 250 PMN Rule: Just like Spontaneous Bacterial Peritonitis, the diagnostic threshold for SBEM is a pleural fluid PMN count >= 250 cells/ml. A positive culture is preferred but not mandatory to initiate immediate treatment if this cellular threshold is crossed.Keep the Chest Tubes Away: Standard purulent empyemas require chest tubes, but Spontaneous Bacterial Empyema does not. Avoid routine chest tube placement to protect your patient from severe, irreversible protein depletion and fatal secondary tract infections.Ceftriaxone is First Line: Initiate empiric treatment immediately with high-dose third-generation cephalosporins. Reserve broader carbapenems or piperacillin-tazobactam for patients presenting in overt septic shock or those with documented multi-drug resistant risks.Bridge to Transplant: SBEM is a definitive marker of severe, advanced liver decompensation (Child-Pugh C). Once the acute pleural infection is successfully cleared, immediately initiate a workup to evaluate the patient for a definitive liver transplant.
0/6