1
Introduction
1 min•111 words
Chest radiography remains the most frequently requested imaging modality in acute medical, surgical, and intensive care settings. Despite its ubiquity, the interpretation of a chest X-ray (CXR) is highly prone to cognitive errors, such as satisfaction of search, where a clinician prematurely halts their evaluation after identifying a single glaring abnormality. To mitigate these diagnostic pitfalls, every healthcare professional must adopt a disciplined, sequential review methodology.
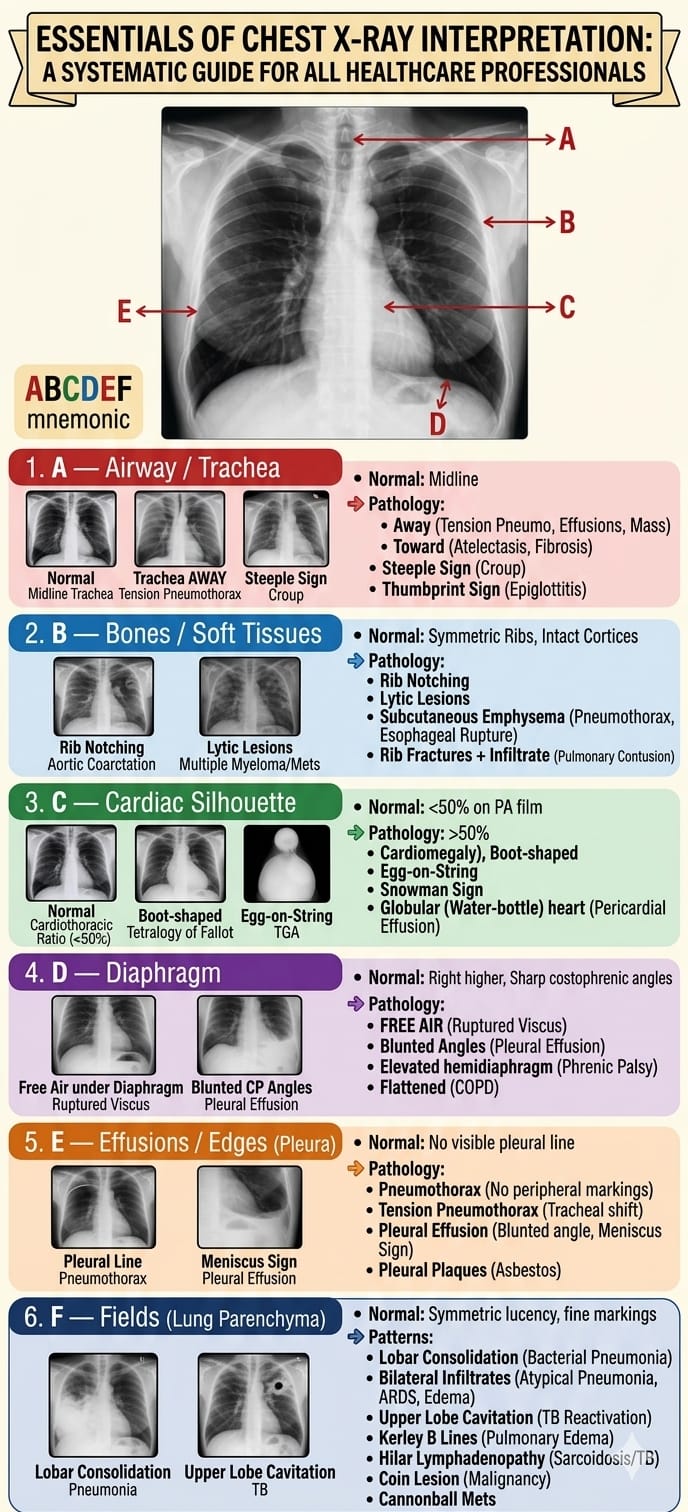
Utilizing a standardized mnemonic like the ABCDEF framework ensures an exhaustive assessment of all anatomical compartments. This sequential protocol transitions the reader systematically from the central airway down through the bony structures, cardiac boundaries, diaphragmatic contours, pleural interfaces, and finally into the lung parenchyma itself.
Utilizing a standardized mnemonic like the ABCDEF framework ensures an exhaustive assessment of all anatomical compartments. This sequential protocol transitions the reader systematically from the central airway down through the bony structures, cardiac boundaries, diaphragmatic contours, pleural interfaces, and finally into the lung parenchyma itself.
2
Background & Pathophysiology
1 min•146 words
Before applying the ABCDEF mnemonic, a clinician must rapidly evaluate the technical adequacy of the radiograph to avoid misinterpreting positional artifacts as true disease processes. This preliminary check relies on assessing three primary variables: rotation, inspiration, and penetration.Rotation is verified by ensuring that the medial ends of both clavicles are equidistant from the spinous process of the adjacent thoracic vertebra. A rotated film artifactually distorts the mediastinum and alters the apparent size of the heart.Inspiration is considered radiographically adequate if the anterior segments of the 6th ribs or the posterior segments of the 9th to 10th ribs are clearly visible above the right hemidiaphragm; poor inspiratory effort crowds the basal vasculature, mimicking airspace disease.Penetration is optimal when the retrocardiac thoracic intervertebral discs are faintly discernible through the central cardiac silhouette. Once technical adequacy is confirmed, the structural mnemonic can be safely executed.The ABCDEF System of Interpretation
3
Key Pearls & Takeaways
1 min•182 words
Stick to the Sequence: Never skip straight to the lung fields. Following the ABCDEF sequence methodically from Airway down to Fields protects the clinician from missing subtle but fatal non-pulmonary findings like free air under the diaphragm.
Know Your Tracheal Shifting Forces: A shifted trachea means a mismatch in intrathoracic pressures. If it is pushed away, think of a space-occupying emergency like a tension pneumothorax. If it is pulled toward, look for parenchymal volume loss like massive atelectasis.
The Meniscus and the Line: Always differentiate peripheral lines. A crisp, vertical line with completely black space devoid of vessels outer to it means a pneumothorax. An upward-curving, dense basilar opacity means a pleural effusion presenting with a meniscus sign.
Look Below the Diaphragm for Surgical Emergencies: A chest X-ray is often the fastest tool to catch an intra-abdominal disaster. Always inspect the subdiaphragmatic space for thin crescents of free air, which confirm a ruptured viscus.
Cavitations Point to TB: In highly endemic regions, an upper lobe thick-walled cavitation on a chest radiograph must be treated as highly infectious pulmonary tuberculosis until proven otherwise.
Know Your Tracheal Shifting Forces: A shifted trachea means a mismatch in intrathoracic pressures. If it is pushed away, think of a space-occupying emergency like a tension pneumothorax. If it is pulled toward, look for parenchymal volume loss like massive atelectasis.
The Meniscus and the Line: Always differentiate peripheral lines. A crisp, vertical line with completely black space devoid of vessels outer to it means a pneumothorax. An upward-curving, dense basilar opacity means a pleural effusion presenting with a meniscus sign.
Look Below the Diaphragm for Surgical Emergencies: A chest X-ray is often the fastest tool to catch an intra-abdominal disaster. Always inspect the subdiaphragmatic space for thin crescents of free air, which confirm a ruptured viscus.
Cavitations Point to TB: In highly endemic regions, an upper lobe thick-walled cavitation on a chest radiograph must be treated as highly infectious pulmonary tuberculosis until proven otherwise.
0/3